

DOI Page / Citation link:
https://doi.org/10.11588/diglit.70004#0145


143
VI. The Contribution of the Missions to Medical Care
With education, medical care has been, and remains, one of the two important
secular activities of the missions. For the Africans, described by the Kenyan
philosopher and theologian J. S. MBITI (1969, 1) as “notoriously religious”,
religion and medicine are traditionally bound together. Thus it was seen as
quite fitting that the missionaries who brought a new faith were also doctors
who healed the sick.
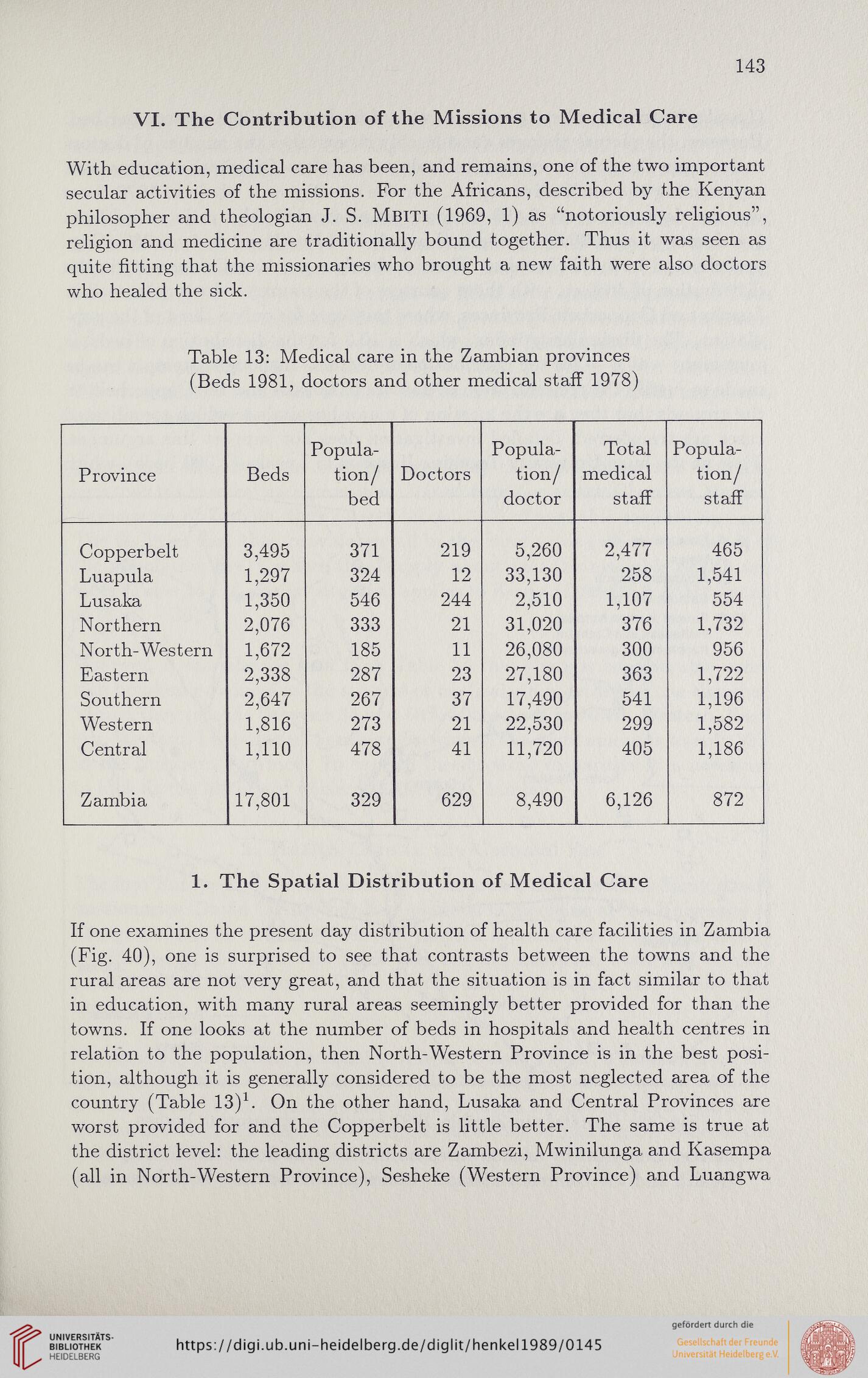
Table 13: Medical care in the Zambian provinces
(Beds 1981, doctors and other medical staff 1978)
Province
Beds
Popula-
tion/
bed
Doctors
Popula-
tion/
doctor
Total
medical
staff
Popula-
tion/
staff
Copperbelt
3,495
371
219
5,260
2,477
465
Luapula
1,297
324
12
33,130
258
1,541
Lusaka
1,350
546
244
2,510
1,107
554
Northern
2,076
333
21
31,020
376
1,732
North-Western
1,672
185
11
26,080
300
956
Eastern
2,338
287
23
27,180
363
1,722
Southern
2,647
267
37
17,490
541
1,196
Western
1,816
273
21
22,530
299
1,582
Central
1,110
478
41
11,720
405
1,186
Zambia
17,801
329
629
8,490
6,126
872
1. The Spatial Distribution of Medical Care
If one examines the present day distribution of health care facilities in Zambia
(Fig. 40), one is surprised to see that contrasts between the towns and the
rural areas are not very great, and that the situation is in fact similar to that
in education, with many rural areas seemingly better provided for than the
towns. If one looks at the number of beds in hospitals and health centres in
relation to the population, then North-Western Province is in the best posi-
tion, although it is generally considered to be the most neglected area of the
country (Table 13)1. On the other hand, Lusaka and Central Provinces are
worst provided for and the Copperbelt is little better. The same is true at
the district level: the leading districts are Zambezi, Mwinilunga and Kasempa
(all in North-Western Province), Sesheke (Western Province) and Luangwa
VI. The Contribution of the Missions to Medical Care
With education, medical care has been, and remains, one of the two important
secular activities of the missions. For the Africans, described by the Kenyan
philosopher and theologian J. S. MBITI (1969, 1) as “notoriously religious”,
religion and medicine are traditionally bound together. Thus it was seen as
quite fitting that the missionaries who brought a new faith were also doctors
who healed the sick.
Table 13: Medical care in the Zambian provinces
(Beds 1981, doctors and other medical staff 1978)
Province
Beds
Popula-
tion/
bed
Doctors
Popula-
tion/
doctor
Total
medical
staff
Popula-
tion/
staff
Copperbelt
3,495
371
219
5,260
2,477
465
Luapula
1,297
324
12
33,130
258
1,541
Lusaka
1,350
546
244
2,510
1,107
554
Northern
2,076
333
21
31,020
376
1,732
North-Western
1,672
185
11
26,080
300
956
Eastern
2,338
287
23
27,180
363
1,722
Southern
2,647
267
37
17,490
541
1,196
Western
1,816
273
21
22,530
299
1,582
Central
1,110
478
41
11,720
405
1,186
Zambia
17,801
329
629
8,490
6,126
872
1. The Spatial Distribution of Medical Care
If one examines the present day distribution of health care facilities in Zambia
(Fig. 40), one is surprised to see that contrasts between the towns and the
rural areas are not very great, and that the situation is in fact similar to that
in education, with many rural areas seemingly better provided for than the
towns. If one looks at the number of beds in hospitals and health centres in
relation to the population, then North-Western Province is in the best posi-
tion, although it is generally considered to be the most neglected area of the
country (Table 13)1. On the other hand, Lusaka and Central Provinces are
worst provided for and the Copperbelt is little better. The same is true at
the district level: the leading districts are Zambezi, Mwinilunga and Kasempa
(all in North-Western Province), Sesheke (Western Province) and Luangwa